
Introduction
The Pregnancy Crisis Helpline is a UK-based charity providing safe and confidential support to those struggling with an unplanned pregnancy or struggling after an abortion.
Visitors to its website are presented with the option of leaving their contact details and a message if they want PCH to get in touch.
This messaging service is enabled using the Zendesk application which stores all messages securely online, accessible only by authorised accounts.
The PCH management team triage all messages as they arrive. They became increasingly concerned about the degree of distress being reported by women contacting the service, and felt it was their duty to examine the data more fully. The PCH Trustees wanted to use this analysis to help shape ongoing team training and to inform the continued refinement of their governance and safeguarding processes, to ensure that the PCH team was fully responsive to all the needs of its callers.
For the purposes of this study, we were provided with a series of messages left by visitors to the PCH website. The analysis for this report is based solely on the content of the initial messages and takes no account of any subsequent, follow-on, contact from a PCH team member with that visitor.
Our study provides insight into how women describe the challenges they face when confronted with an unplanned pregnancy, how she describes her situation, circumstances, thoughts, and feelings – in her own words – before she has any contact with the pregnancy support team.
Materials and Methods
PCH management gave the research team time-limited online access to the Zendesk administration portal, from which we were able to download the message records from August 2021 to December 2023. From each record, we extracted only the data that was necessary for this study, ensuring that no personal identifiable data was taken. The data extracted were the unique anonymised identifier created by Zendesk for each message, the message text in full, and the month in which the message was received. The dataset comprised a complete sequence of 1,159 messages across 29 months.
The extracted records were copied into a spreadsheet using Microsoft 365 Excel; all further work on these records was completed using Excel, including the allocation of each message to its selected category and the analysis of the results.
Messages, for the full sequence, were reviewed one-by-one and based on the content of the message, possible category codes were added to each record. This was repeated until the working set of categories was sufficient for each subsequent message. Nine category codes were chosen and each of the 1,159 messages were allocated to the single category which we considered a best fit.
It would be appropriate to group these nine categories into two groups, the first being messages best handled by the PCH Office Management team, and the second being those for which the PCH Helpers are trained – contact from women wanting help with a crisis pregnancy or post-abortion distress.
Group 1: PCH Office Management
Office Manager – messages that were best answered by the PCH Office Manager. Some were requests for information about PCH, some were from existing clients asking to be called back by a named team member, and a few were enquiries about how to become a volunteer at PCH.
Requesting abortion – messages in which the visitor was requesting an abortion, many explicitly asking for pills-by-post. The visitors had either not read or had chosen to ignore the notice on the PCH website that says: “Please note: we do not refer for abortion or offer medical advice.” [our emphasis]
No information provided – messages in which the visitor was simply reaching out, asking for a call or contact. Some were very brief, nothing more than a ‘hello’, perhaps just trying to see if anybody would engage online. These messages did not include any information indicating why contact was being made and so could not be categorised any further. As noted above, this study was limited to analysis of the initial message only. If we were to review the follow-on for these ‘No Information Provided’ messages, it is likely that some would subsequently fall into one of the categories in Group 2.
Medical advice – messages from visitors asking for help and advice related to health aspects of their pregnancy. Some asking for help to clarify conflicting results from pregnancy tests, some had questions about sex and/or contraception, a few were from young women worried about becoming pregnant after having sex without using contraception; others mentioned concerns about spotting, bleeding, or abdominal pain. As noted above, PCH clearly states on its website: “Please note: we do not refer for abortion or offer medical advice.” [our emphasis] and, more relevantly, on the Zendesk chat box it says: “Please note: we do not offer medical advice”.
Group 2: PCH Helpline Team
There are two sets of messages in Group 2, the first are from women struggling with pregnancy decisions and the second from those who have issues arising from having had an abortion.
Set 1: Struggling with pregnancy decisions
Reason not specified – messages in which the visitor indicated that she was struggling to decide which option was best for her – to continue with her pregnancy or to have an abortion. Often these messages indicated that she wanted PCH to help her to decide what she should do. The initial message did not give us enough information to be sure of allocating it into one of the more specific categories below, but from our analysis of all the messages in the following categories, it is likely that after further discussion with a woman leaving these ‘Struggling…’ messages, we might find the cause of that struggle to be Internal conflict, Coercion by partner or family, or Pressure from difficult circumstances.
I’ve just found out that I’m pregnant, I’m scared and I’m struggling to know what decision is the right one for me, to keep the baby or to have an abortion. I don’t know who to talk with, there are so many factors in my life, I’m feeling overwhelmed, it’s all too much for me right now, please can I speak to someone today? [i]
Internal conflict – messages in which the visitor expressed the internal tension of not knowing what to do for the best. Difficult circumstances and advice from those around her were causing her to consider abortion but she was not sure that she could live with herself if she did that. Many expressed worry and concern that they might end up regretting it later, often indicating that abortion was against their internal values.
Coercion by partner or family – messages in which the visitor explicitly mentioned that she was being persuaded or forced by her partner or family member to get an abortion, but that she did not want to do so, saying that abortion would not be her preferred choice.
Pressure from difficult circumstances – messages in which the visitor said that her difficult circumstances did not seem to be compatible with having a baby at that time e.g., worries and concerns about relationship problems, financial pressures, unsuitable housing, inconvenient timing for her work or education, and health issues. She expressed a feeling that these were making her lean towards having an abortion even though doing so would not be her preferred choice.
Set 2: Post-abortion distress
Messages in which the visitor described difficult emotions or troubling thoughts following an abortion and asked for help to work through these. Some were making contact just days or weeks after their abortion, others described having carried the pain for many years, even decades, often without having told anyone about it.
Several reviews of the full series of messages were undertaken before finally settling on the above categories. In between these iterative rounds, the lead researcher discussed the emerging results with the PCH Trustees, testing the suitability of each chosen category with a set of sample messages. These discussions helped to shape the final choice of categories and the criteria by which messages were allocated to each; we chose to allocate each message to just one category, based upon our assessment of the best fit. Of course, the research team recognises and accepts that another reviewer might on occasion choose a different message categorisation.
Results
| GROUP 2 | |
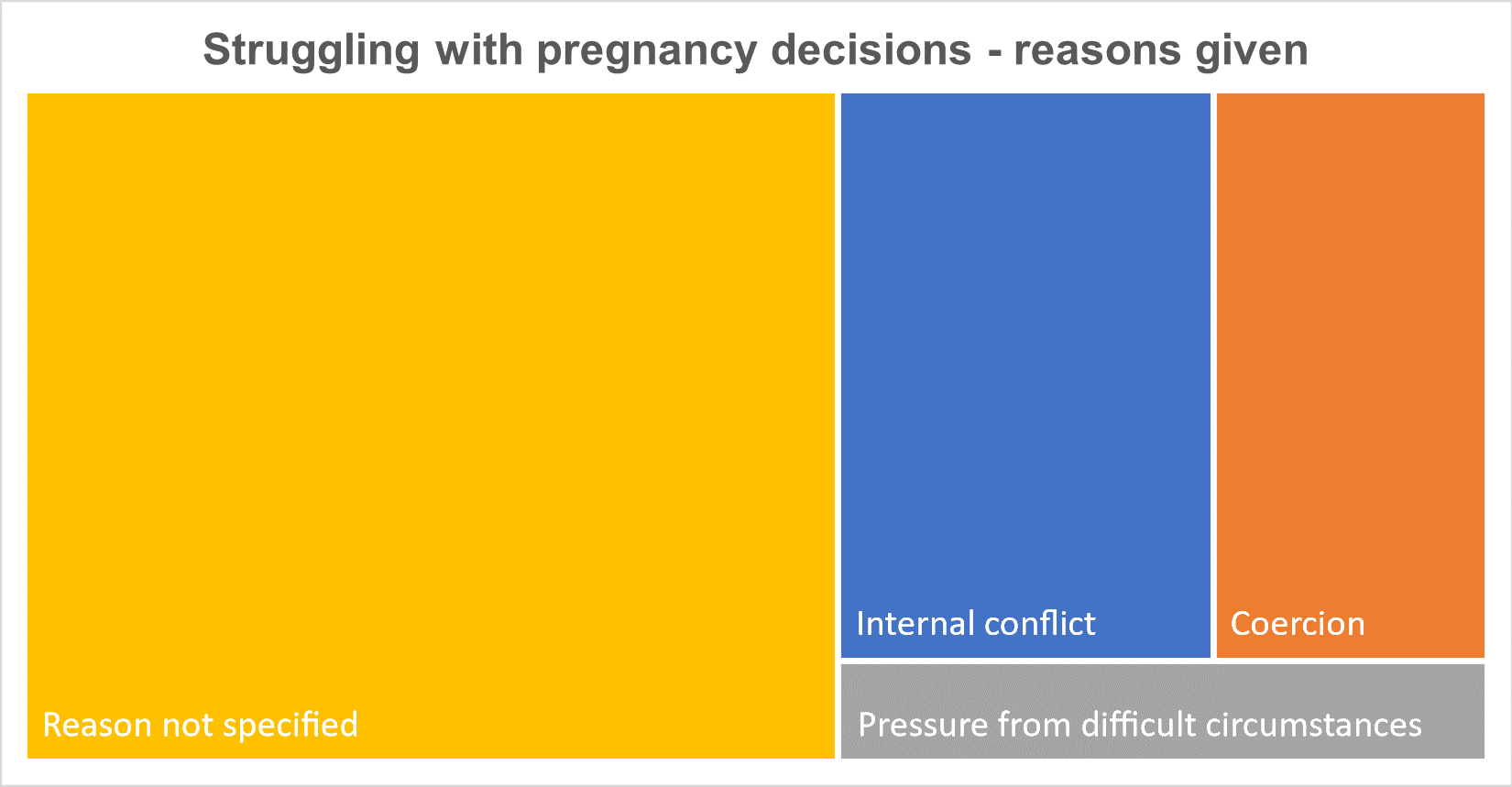
| Struggling with pregnancy decisions | 358 (70%) |
| Internal conflict | 78 (22%) |
| Coercion by partner or family | 57 (16%) |
| Pressure from difficult circumstances | 24 (7%) |
| Reason not specified | 199 (55%) |
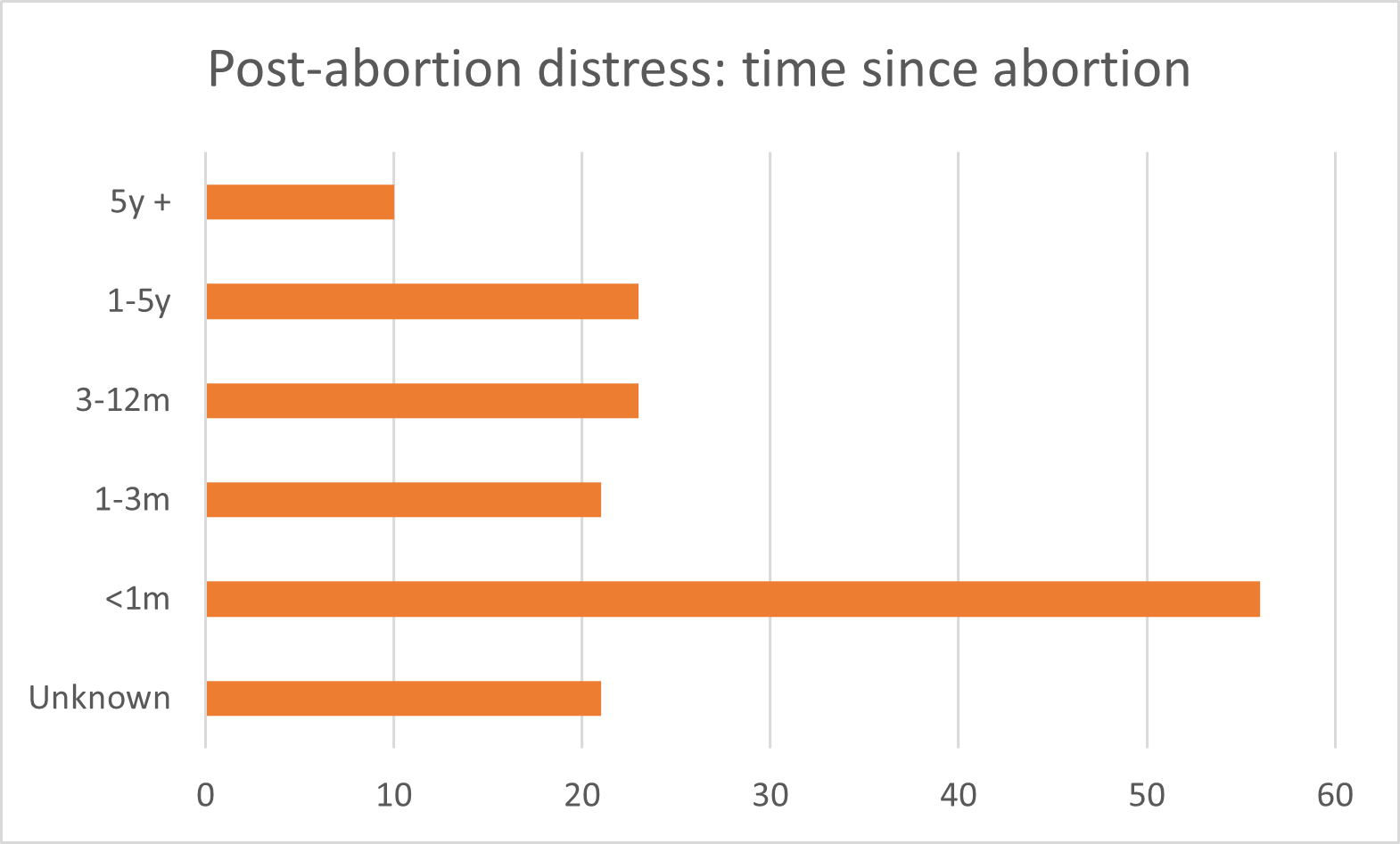
| Post-abortion distress | 154 (30%) |
| Less than 1 month | 56 (36%) |
| 1 month up to 3 months | 21 (14%) |
| 3 months up to 1 year | 23 (15%) |
| 1 year up to 5 years | 23 (15%) |
| 5 years to 30+ years | 10 (6%) |
| Unknown | 21 (14%) |
The full sequence of messages totalled 1,159.
For the purposes of this study, the 647 messages in Group 1, (allocated to the categories Office Manager, Requesting abortion, No information provided, and Medical advice), were set aside.
The remaining 512 messages, in Group 2, were from women who reached out to the Pregnancy Crisis Helpline because they were struggling with pregnancy decisions or with issues arising from having had an abortion.
Discussion
When designing this study, we were interested in gaining a better understanding of how women describe the challenges they face when confronted with an unintended, unplanned, or unwanted pregnancy. We wanted to hear this in her own words, those by which she describes her situation, circumstances, thoughts, and feelings, before she has any contact with a pregnancy support team.
We are often reminded how common, and even normal, it is for a woman to have an abortion, and that as many as one-in-three women have chosen to do so. Of course, this does not mean that it is always an easy decision for these women; in its online information for those considering an abortion, the Royal College of Obstetricians and Gynaecologists (RCOG) says: “For most women the decision to have an abortion is not easy.” [ii]
This set of 512 messages over 29 months is a small sample, especially in the context of more than 400,000 abortions over the same period. Whilst we cannot extrapolate our findings to the population of all women presenting for an abortion, we do consider these messages to be indicative of the many women who find themselves facing the difficult choice about whether to continue with their pregnancy or not.
Struggling with pregnancy decisions
We chose to allocate some messages to the ‘Struggling with pregnancy decisions’ category simply because ‘struggling’ was the word used by so many of the women whose messages we were reading. Women told us how they were struggling to deal with an unplanned pregnancy and were finding it difficult to decide what would be best for them- to either continue with the pregnancy or to have an abortion. They described how they were overwhelmed with emotions and thoughts about this, using words like ‘confused’, ‘uncertain’, ‘anxious’, ‘scared’ and even ‘terrified’; though as mentioned above, these messages were not specific enough for the research team to confidently allocate to one of the following categories, hence our use of the label ‘Reason not specified’. Many said they were getting in touch with PCH because they needed to talk with someone and wanted help with making that decision. Some qualified that further as making the ‘right decision’; for these women their abortion decision is not simple or easy – and so they are proactively seeking help and want to talk it through with somebody.
Internal conflict
The next set of messages, ‘Internal conflict’, reveals more about how women want to make the choice that is right for them. As we described above, these are messages in which the woman expressed an internal tension from not knowing what to do for the best, the best being, in her own words, a decision that she would not later find herself regretting. These women were clearly struggling and provided more context for that struggle by sharing their difficulty in choosing abortion. They described the circumstances or reasons why they were leaning towards having an abortion, whilst at the same time admitting not being certain if they could live with such a decision. Even in these initial messages, before they have spoken with a member of the PCH team, these women are telling us about how they are troubled by even thinking about having an abortion, and how this was something that they had always thought would not be for them.
I’ve recently found out that I am pregnant and I’m very conflicted with what to do, whether to keep my baby or get an abortion. Others think an abortion is a good idea but something inside me wants to keep the baby. It’s not great timing, I really don’t know how I would cope with being a mum but I just feel really sick at the thought of abortion and know that I would regret it and feel guilty forever.
To respect the privacy of women contacting PCH and to protect their identity, we have chosen not to quote directly from any of their messages but instead to paraphrase from a number of similar messages to present the reader with an example of a typical message for a specific category. A typical message from women in the category ‘Internal conflict’ reads like this: “I don’t want an abortion, I’ve always wanted to be a mum but I don’t see how I can have the baby at this time, in my current situation, but I’m worried that I will feel guilty and regret having an abortion. I don’t know what to do for the best, please help me.”
These women know in themselves, and they are telling us, that abortion is very much a values-loaded choice, and that their internal values matter.
Coercion by partner or family
Women are not always free to make their own choice about abortion. Many feel pressured by their circumstances, whilst others are victims of reproductive coercion. We chose to categorise some messages as ‘Coercion by partner or family’ because that is a term used by experts when referring to breaches of abortion legislation. Reproductive coercion was included in the set of illegal behaviours described as “coercive control” in the Serious Crime Act 2015, though it is important to recognise that whilst many women are coerced into abortion, very few cases are ever investigated.
A Savanta ComRes poll commissioned by the BBC in February 2022, found that 15% of women aged 18-44 had been pressured into having an abortion they did not want; 85% by an intimate partner and 11% by a close family member. [iii]
In his report for clinicians, published by the British Medical Journal, Professor Sam Rowlands described reproductive coercion as “any deliberate attempt to dictate a woman’s reproductive choices or interfere with her reproductive autonomy. It comprises a range of behaviours, from psychological pressure through to threats of (and actual) physical and sexual violence.” He gives this as an example of reproductive coercion behaviour: “Emotional blackmail/threats or other coercion to force a woman to have a termination of pregnancy.” [iv]
The Department of Health and Social Care (DHSC) has set out legislation that must be followed by every abortion provider, the details of which are to be found in the required standard operating procedures (RSOPs).[v] RSOP 10, explains the law regarding consent, stating that a woman’s consent must be provided voluntarily and without undue pressure on her to accept or refuse treatment. The NHS explains the meaning of voluntary as: “the decision to either consent or not to consent to treatment must be made by the person, and must not be influenced by pressure from medical staff, friends or family.” [vi]
When I told my partner I was pregnant, he said I needed to get an abortion. But I don’t want an abortion – I don’t think that I could go through that again. He gets angry though, and if I keep it, I’m worried that he’ll kick me out of the house or get violent again.
RSOP 3 states that abortion providers are obliged to provide additional safeguarding support for women “who may be experiencing sexual and/or domestic violence and abuse (physical and emotional), including where there is evidence of coercion.”
The words ‘coercion’ or ‘coerce’ or ‘coerced’ were only used by two women across all 1,159 messages; in one the woman mentions that she had read a lot about this when trying to come to terms with an abusive relationship and the other is from a woman writing about her abortion ten years ago. Whilst the other messages do not use the word ‘coerced’, women are very clear in these messages that they are being persuaded or forced by a partner or family member into having an abortion that they themselves do not want. They often share how they are being ‘pressured’ or ‘made to’, ‘pushed into’, or ‘forced to’. These women tell us: “he doesn’t want it and says I must get rid of it or else.” Many go on to describe what that ‘or else’ means; often it includes the threat of, or actual, violence, abandonment or being ‘kicked out’ of their home. They tell us that they want to keep their ‘baby’, that they do not want to have an abortion, but they feel they have no choice in the matter and are finding it very difficult to see some other way out of this. In some of these messages, women share their concerns that, if they give in to the pressure to abort, they will then be living with guilt and regret.
It is a legal requirement, as stated in RSOP 8, for all abortion providers to have robust processes and governance in place to ensure that women are willingly and freely, of their own accord, consenting to an abortion, and to be sure of the absence of any coercion or otherwise escalate to their safeguarding team, before proceeding with the abortion.
Pressure from difficult circumstances
A smaller group of women told us how ‘pressure from difficult circumstances’ was causing them to lean towards an abortion decision, the pressure coming from e.g., difficulties in the relationship with their partner, the inconvenient timing of this pregnancy, perhaps they have just started university, or not wanting to exacerbate current job insecurities. Many of these women mentioned concerns about money, and we know from statements made by the British Pregnancy Advisory Service (BPAS) that financial pressure often forces women to have an abortion.
In June 2023, commenting on the unprecedented increase in the number of abortions, (a 17% increase in the first six months of 2022 compared with the same period in 2021), BPAS cited financial pressures, including “the impact of interest rate hikes and the huge increase in the cost of living”, as being a key driver in women’s abortion decisions. BPAS, whilst noting that “Unplanned pregnancies are not always unwanted”, stated that during abortion consultations, many women were saying “that the circumstances they are in mean it is simply not the right time to start or expand a family.” [vii]
In August 2023, a BPAS spokesperson addressing the financial pressure on pregnant women, said: “…many women experiencing an unplanned pregnancy will tell BPAS that they want to start or expand their families but feel unable to do so because money is so tight at the moment.” [viii] An earlier statement, in April 2023, stated quite bluntly that financial worries ‘force’ women to have an unwanted abortion: “Unfortunately, financial struggles and a lack of government support, including the two-child limit on financial assistance, continue to force women to choose between ending an otherwise wanted pregnancy or plunging their families in to great hardship.” [ix]
I know it’s bad timing and that I’ll struggle financially but I don’t know if I could go through with an abortion, at times it just seems like the best idea but I really don’t want to do it. I’m starting to bond with the baby but I just can’t see a way forward. I feel trapped, what should I do?
This is exactly what women are saying to us in these messages. In describing the source of their particular pressure, women say that they do not want to have an abortion, that it would not be their preferred choice but given their current situation they cannot see any alternative; they are feeling pressured by financial worries into having an abortion that they would prefer not to have.
Post-abortion distress
154 messages were from women asking for help in dealing with troubling thoughts and emotions following an abortion. We categorised these as ‘Post-abortion distress’.
In its online information for women considering an abortion, the Royal College of Obstetricians and Gynaecologists notes that a few women might continue to experience ‘distress’ in the weeks following their abortion. Addressing the long-term effects of abortion, they say: “For most women the decision to have an abortion is not easy. How you react will depend on the circumstances of your abortion, the reasons for having it and how comfortable you feel about your decision…; long-term feelings of sadness, guilt and regret appear to linger in only a minority of women.” [x]
This very much reflects what women are telling us. They use the same words: ‘sadness’, ‘guilt’ and ‘regret’, sometimes saying they are filled with ‘grief’ when thinking about the ‘loss of their baby’, often noting that they had not been comfortable with their decision at the time, feeling pressured by circumstances or coerced by a loved one.
Just over a third of the women reaching out to PCH for help with their post-abortion distress told us that their feelings were still very raw, their abortion having been very recent, no more than a day to about a month ago.
Others, whose abortion had been more than a month ago, were getting in touch because, as they outlined in their messages, unwelcome thoughts and emotions about their abortion had continued or had been triggered by recent events, perhaps the anniversary of the aborted baby’s due date or being around others celebrating their pregnancy or a child’s birthday. Fifteen percent of the women reaching out for help with post-abortion distress had carried their hurtful memories for more than one year, and a further six percent said their abortion had been more than five years ago, with a few indicating ten, twenty, or thirty years; these are the women for whom RCOG says long-term feelings of distress linger.
Many of the women contacting PCH with post-abortion distress share in their own words how they have been affected and how they made their abortion decision because of pressure from loved ones, financial concerns, or other difficult circumstances. In some of these messages, we read how their abortion has had a traumatic effect on their mental health; women tell us about their difficulties in getting back into the flow of normal life, their trouble functioning well at work, how they are having vivid flashbacks and dreams, and a few refer to panic attacks.
I had an abortion a year ago. I didn’t want to go through with it but the pressure from my husband and family members made me do it. I have flashbacks and nightmares and keep crying; it’s coming up to what would have been the first birthday and I’m filled with regret that I wasn’t strong enough to make the decision I wanted. Life has lost all its colour. I just wish I could go back in time, I’ve tried to forget and move on but I can’t. Is there anyone who can offer support?
Their descriptions of worrying thoughts and emotions, and how these at times impact on their daily lives, is consistent with the findings in a paper published by Cureus in 2023 from David Reardon and Tessa Longbons. [xi] Their research shows that a perceived pressure to abort was significantly associated with more negative emotions; more disruption of daily life, work, or relationships; more frequent thoughts, dreams, or flashbacks to the abortion; more frequent feelings of loss, grief or sadness about the abortion; more moral and maternal conflict over the abortion decision; a decline in overall mental health that they attribute to their abortions; and more desire or need for help to cope with negative feelings about the abortion.
Many say that the decision to have the abortion was not what they wanted, it was not their preferred choice and at the time they knew this would be in conflict with their own internal values but they had been coerced by others or felt trapped by their difficult circumstances. In a related paper, about the same study, Reardon writes: An additional categorical question was asked: “Which best describes your abortion decision?” Respondents were presented with four possible answers: “Wanted and consistent with my values and preferences,” (Wanted), “Accepted but inconsistent with my values or preferences” (Inconsistent), “Unwanted and contrary to my values and preferences” (Unwanted) or “Coerced and contrary to my values and preferences” (Coerced). [xii]
He found that women who experienced their abortion as a violation of their own values and preferences, (Inconsistent, Unwanted and Coerced), were more likely to attribute an overall negative effect on their mental health to their abortions, have more moral and maternal conflicts over their abortion decision, and be less confident in the rightness of their decision. It is worth noting that these women were more likely to report that they would have given birth if they had received more support from others and/or had more financial security.
Based on our reading of these messages and the above noted research of others, our hypothesis is that women who are not able to make their own preferred decision, consistent with their own personal values – so those who have internal conflict, are suffering coercion by a partner or family, or are feeling pressure from difficult circumstances – are likely to be the ones who will suffer lingering post-abortion distress.
Conclusions
These findings raise questions about how women are reaching their decision to have an abortion, and whether these decisions are their preferred choice, or have been influenced by pressure from circumstances or others. If the latter, then legal consent has not been given voluntarily and without undue pressure, as required in the regulations.
Our society seems to suggest that every abortion choice is the right choice. But the messages in this study suggest something different. Some women come to recognise that they are suffering from post-abortion distress and many of these women can connect this with having had an abortion that they did not want.
The data suggests that we should review both the safeguards in place to protect women in these highly pressured circumstances, and the governance processes of abortion providers that are supposed to ensure that these safeguards are being followed.
We suggest that further research is needed to inform the design of better counselling and support for women facing difficult decisions about whether to have an abortion, so that these vulnerable women are empowered to make fully informed choices and safeguarded from making decisions that they might later regret.
I would like to say a massive thank you … for the call last night, it really helped… it was refreshing to talk to someone new and not to be judged. Thank you for your help.
You can download a PDF of this report here…
[i] To respect the privacy of women contacting PCH and to protect their identity, we have chosen not to quote directly from any of their messages but instead to paraphrase from a number of similar messages to present the reader with an example of a typical message for a specific category.
[ii] RCOG – Patient Information – Abortion care. https://www.rcog.org.uk/for-the-public/browse-our-patient-information/abortion-care/
[iii] Savanta ComRes. Reproductive coercion poll – BBC Radio 4 – 8 March 2022. Published December 16, 2022. https://savanta.com/knowledge-centre/poll/reproductive-coercion-poll-bbc-radio-4-8-march-2022/
[iv] Rowlands S, Holdsworth R, Sowemimo A. How to recognise and respond to reproductive coercion. The BMJ. Published online September 20, 2022. doi:10.1136/bmj-2021-069043
[v] Procedures for the approval of independent sector places for termination of pregnancy (abortion) in England. GOV.UK. Published March 27, 2023. https://www.gov.uk/government/publications/update-to-procedures-for-the-approval-of-independent-sector-places-published/procedures-for-the-approval-of-independent-sector-places-for-termination-of-pregnancy-abortion-in-england
[vi] NHS. Consent to treatment. nhs.uk. Published August 22, 2023. https://www.nhs.uk/conditions/consent-to-treatment/
[vii] BPAS. New government figures show 17% rise in abortions. Published June 22, 2023. https://www.bpas.org/about-bpas/press-office/press-releases/new-government-figures-show-17-rise-in-abortions/
[viii] BPAS. Number of births in England and Wales continues to decrease – ONS report. Published August 17, 2023. https://www.bpas.org/about-bpas/press-office/press-releases/number-of-births-in-england-and-wales-continues-to-decrease-ons-report/
[ix] BPAS. BPAS comment on ONS conception rates. Published April 04, 2023. https://www.bpas.org/about-bpas/press-office/press-releases/bpas-comment-on-ons-conception-rates/
[x] RCOG – Patient Information – Abortion care.
[xi] Reardon DC, Longbons T. Effects of pressure to abort on women’s emotional responses and mental health. Cureus. Published online January 31, 2023. doi:10.7759/cureus.34456
[xii] Reardon DC, Rafferty KA, Longbons T. The effects of abortion decision rightness and decision type on women’s satisfaction and mental health. Cureus. Published online May 11, 2023. doi:10.7759/cureus.38882
